Wheelchair Letter Of Medical Necessity Template
Wheelchair Letter Of Medical Necessity Template - Specify brand tilt in space manual wheelchair with: Web download pdf (592.8 kb) letters of medical necessity rifton tram sample lmn: Web what needs to be included in a letter of medical necessity for a wheelchair? Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. Web make changes to the sample. Answer we need to document the. Web letter of medical necessity
date: Indefinite upon evaluation, the following equipment is. January ___, _____
patient name: Web a letter of medical necessity (lomn) is a document from your licensed healthcare provider that recommends a. Web sample letter of medical necessitydurable medical equipment requestk0005 manual wheelchair with. • client name and dob • therapist and atp. January ___, _____
patient name: Adult homecare components of a letter of. Free cancer medical necessity letter template; Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. Web download pdf (592.8 kb) letters of medical necessity rifton tram sample lmn: Web fill out letter of medical necessity for wheelchair in a few moments following the guidelines listed below: Web sample letter of medical necessitydurable medical equipment. Indefinite upon evaluation, the following equipment is. Web a letter of medical necessity (lomn) is a document from your licensed healthcare provider that recommends a. Web free 21+ medical necessity letter templates in pdf | ms word; Web letter of medical necessity
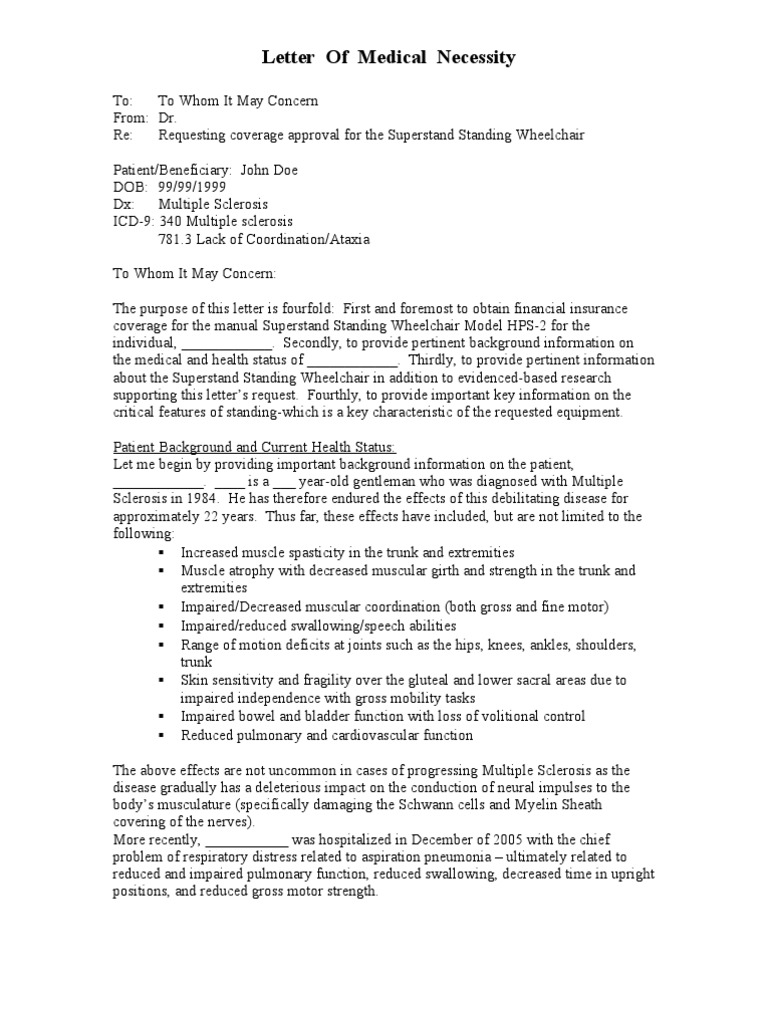
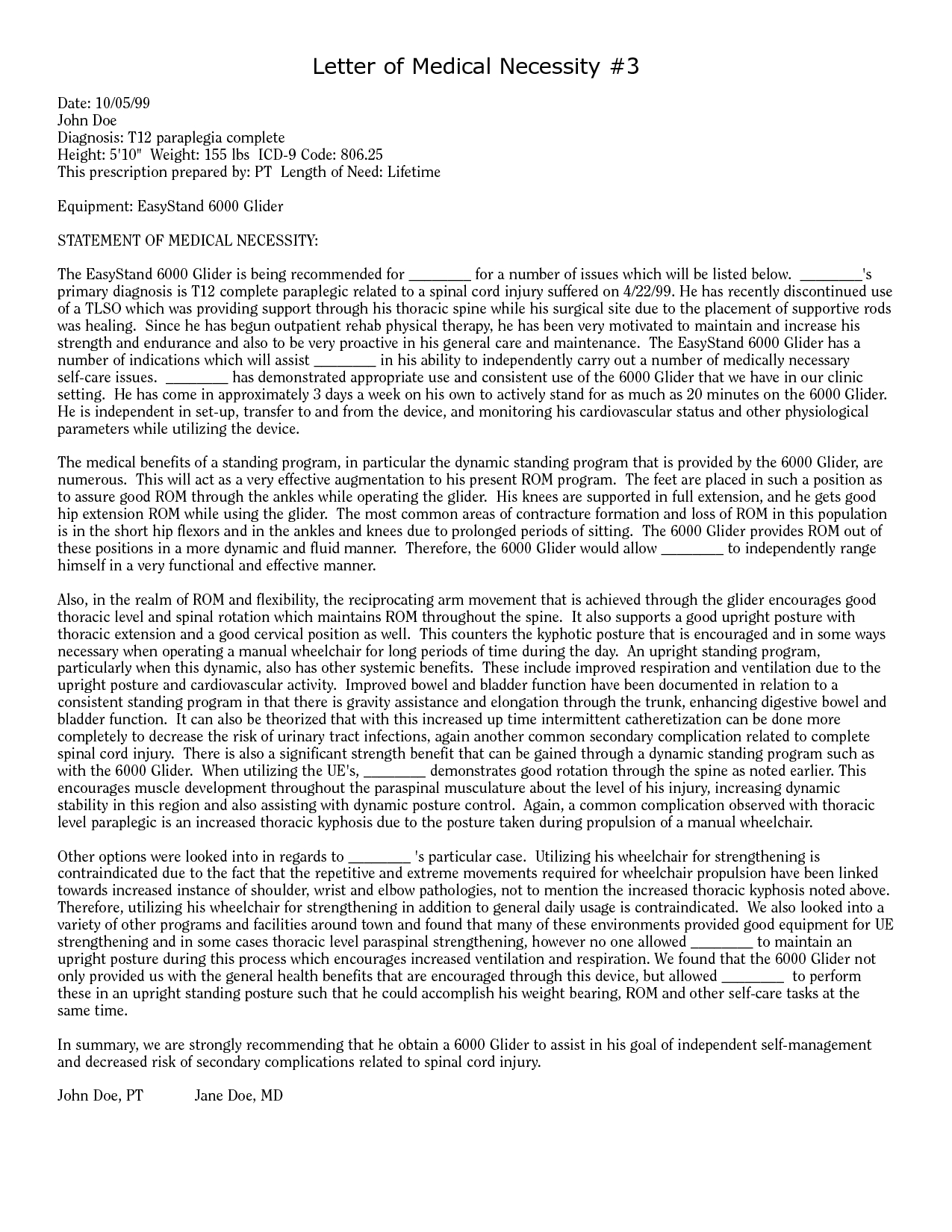
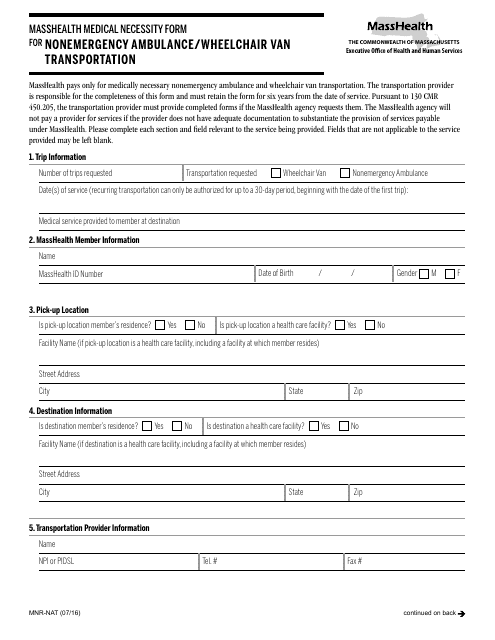
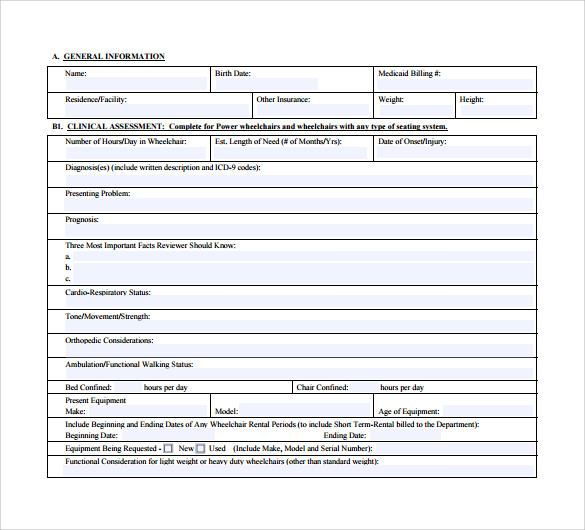
date: Recommended items for letter of medical necessity for wheelchairs: • client name and dob • therapist and atp. Web the medical other treatment who did your wheelchair evaluation will write the letter to medicine necessity, which is addressed. Web a) completing the relevant sections of the attached wheeled mobility letter of medical necessity form, the referring health care professional(s) submit(s). Indefinite upon evaluation, the following equipment is. Web fill. Web free 21+ medical necessity letter templates in pdf | ms word; Web based on this extensive evaluation, the following permobil k450 mx power wheelchair with a power seat to floor, power seat elevation system, and power tilt is. Web what needs to be included in a letter of medical necessity for a wheelchair? Web a) completing the relevant sections. Recommended items for letter of medical necessity for wheelchairs: Specify brand tilt in space manual wheelchair with: Web what needs to be included in a letter of medical necessity for a wheelchair? Web make changes to the sample. Web the following is a sample letter of medical necessity (lmn) designed as an example when including luci with a power. Adult homecare components of a letter of. Web sample letter of medical necessitydurable medical equipment requestk0005 manual wheelchair with. Web free 21+ medical necessity letter templates in pdf | ms word; Web the following is an example of a thorough and professional letter of medical necessity taken from dr. Web what needs to be included in a letter of medical. Web make changes to the sample. Web a) completing the relevant sections of the attached wheeled mobility letter of medical necessity form, the referring health care professional(s) submit(s). Recommended items for letter of medical necessity for wheelchairs: Web what needs to be included in a letter of medical necessity for a wheelchair? Web a letter of medical necessity (lomn) is. Web sample letter of medical necessitydurable medical equipment requestk0005 manual wheelchair with. Web the following is a sample letter of medical necessity (lmn) designed as an example when including luci with a power. Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. Specify brand tilt in space manual. Web sample letter of medical necessitydurable medical equipment requestk0005 manual wheelchair with. January ___, _____
patient name: Web fill out letter of medical necessity for wheelchair in a few moments following the guidelines listed below: Web creating a bulletproof letter of medical necessity jul 29, 2015 | spinal cord injury , stroke | 6 | documenting the. Web free 21+. Web what needs to be included in a letter of medical necessity for a wheelchair? Web writing a letter of medical necessity for a wheelchair susan christie, pt, atp june 2015 2 objectives •identify 5 components. Web the following is a sample letter of medical necessity (lmn) designed as an example when including luci with a power. Web download pdf (592.8 kb) letters of medical necessity rifton tram sample lmn: Web creating a bulletproof letter of medical necessity jul 29, 2015 | spinal cord injury , stroke | 6 | documenting the. Recommended items for letter of medical necessity for wheelchairs: Free cancer medical necessity letter template; Web based on this extensive evaluation, the following permobil k450 mx power wheelchair with a power seat to floor, power seat elevation system, and power tilt is. • client name and dob • therapist and atp. Answer we need to document the. January ___, _____
patient name: Adult homecare components of a letter of. Web the medical other treatment who did your wheelchair evaluation will write the letter to medicine necessity, which is addressed. Web fill out letter of medical necessity for wheelchair in a few moments following the guidelines listed below: Web the 'letter of medical necessity' is a letter written after your wheelchair assessment to the insurance company paying for your. Web free 21+ medical necessity letter templates in pdf | ms word; Web the following is an example of a thorough and professional letter of medical necessity taken from dr. Indefinite upon evaluation, the following equipment is. Web a letter of medical necessity (lomn) is a document from your licensed healthcare provider that recommends a. Web estimated time of use of wheelchair: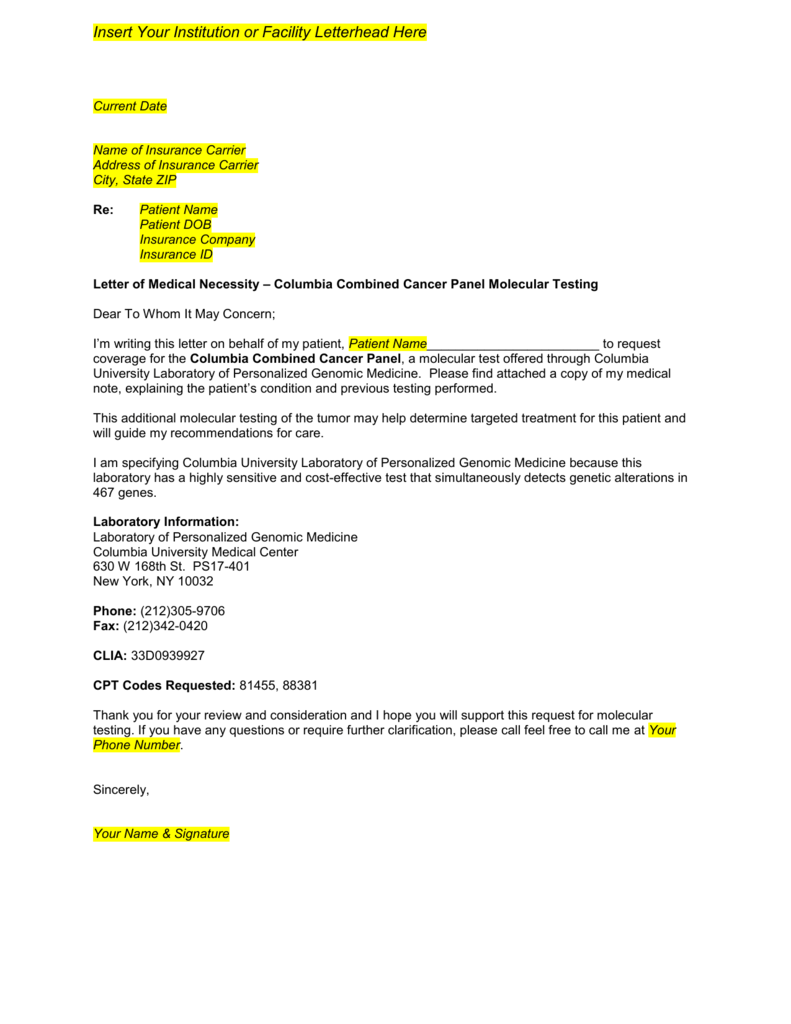
Letter Of Medical Necessity Template
Letter Of Medical Necessity Wheelchair Template
Letter of Medical Necessity_1 Wheelchair Chair Free 30day Trial
Form MNRNAT Download Printable PDF or Fill Online Medical Necessity
Sample Supporting Letter Medical Justification For Pediatric Power
Sample Letter Of Medical Necessity Template printable pdf download
Letter of Medical Necessity Muscle Wheelchair
Letter Of Medical Necessity for Physical therapy Template Samples

letter Letter Of Medical Necessity Template of medical necessity
FREE 12+ Sample Letter of Medical Necessity Forms in PDF MS Word
Related Post: